2026-27 California health budget guide: Medi-cal updates, cuts, coverages, and timelines
California's 2026-27 budget spares Medi-Cal from immediate cuts—but sets almost every painful decision on a timer. Here's what's funded now, what disappears in July 2027, and what the next governor must decide.


The strategy: Delay the Medi-Cal cuts to 2027
Roughly one in three Californians relies on Medi-Cal, and this was the year the program's finances were supposed to crack. Federal cuts under H.R. 1 threaten tens of billions of the roughly $187 billion in federal funds that flow through California's budget, Medi-Cal costs have ballooned, and Governor Newsom's January proposal sketched cuts that would have reshaped the program immediately.
The final budget, signed June 29, does something different: it buys a year. Nearly every major reduction—dental benefits, clinic payments, immigrant coverage, the asset test—now takes effect July 1, 2027, six months after Newsom leaves office. The Legislature rejected a handful of cuts outright, funded targeted priorities, and papered over the rest with a renewed tax on health plans and the hope that AI-driven revenues hold.
"This is a budget that bought time," Sen. María Elena Durazo, a Los Angeles Democrat, said before the final vote. "Medi-Cal delayed, not resolved, not restored."
This guide walks through what that means in practice: what's funded now, what changes on each date between now and July 2027, and the decisions that were deliberately left for California's next governor.
What's funded now: Hospitals, Covered California, HIV prevention
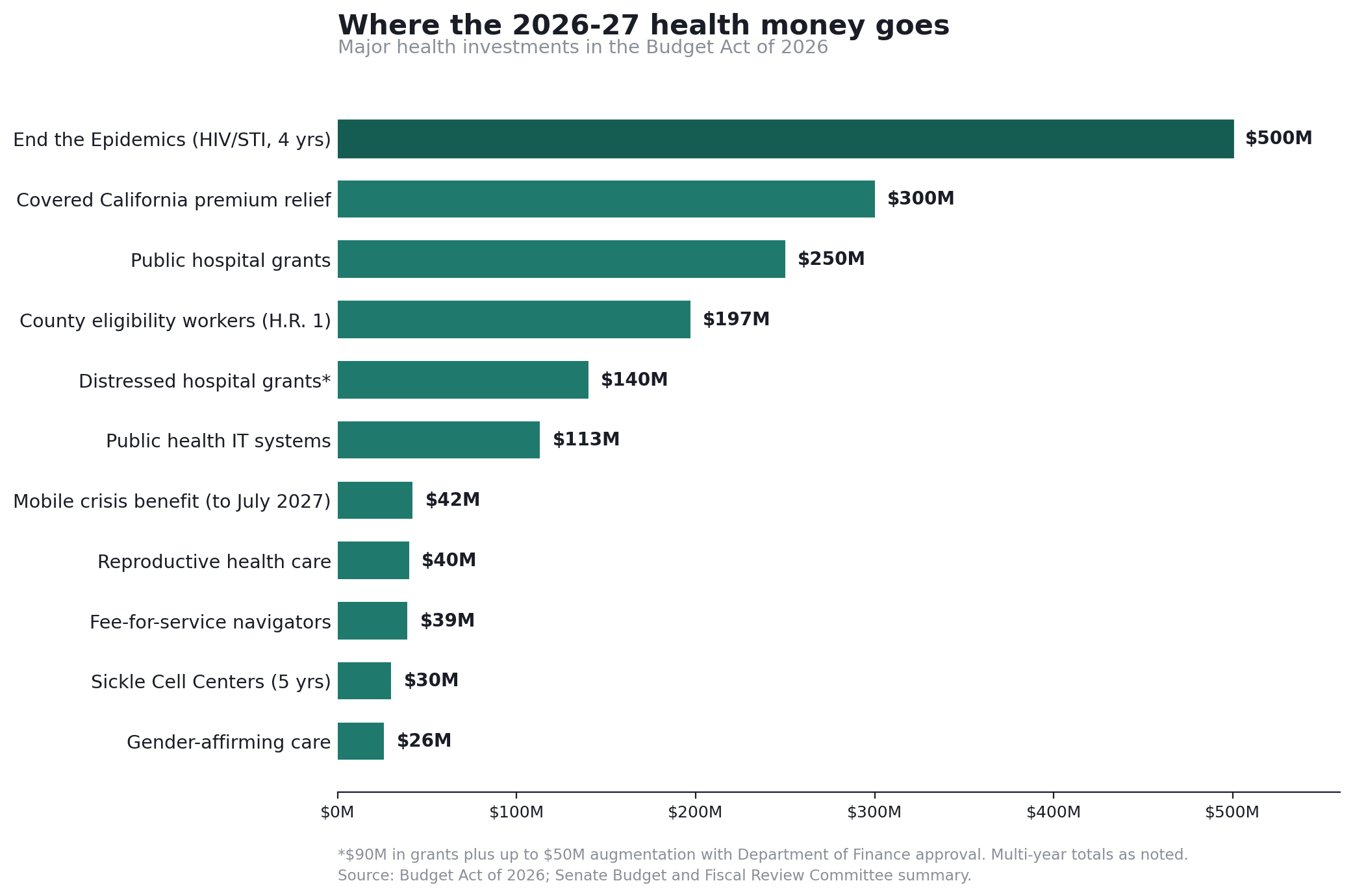
The 2026-27 spending side is real, and some of it is substantial:
- Public hospitals: $250 million in grants to designated public hospitals—structured so the money doesn't offset other state obligations. Hospital groups had asked for $500 million as federal cuts squeeze their finances.
- Distressed hospitals: $90 million in grants for hospitals in significant financial distress, which the administration can augment by up to $50 million, plus $10 million for a new unit that evaluates struggling hospitals and helps them stay open.
- Covered California: $300 million to cut premiums for low- and middle-income enrollees—erasing premiums entirely for the lowest-income and trimming out-of-pocket costs for middle-class households, a Newsom priority as federal subsidies lapse.
- End the Epidemics: nearly $500 million over four years for HIV/AIDS and STI programs, funded from AIDS Drug Assistance Program rebate funds—including a syphilis outbreak strategy targeting the elevated rates in Fresno, Sacramento, and Kern counties.
- County eligibility workers: $197 million so counties can process the more frequent eligibility checks H.R. 1 requires—the administrative machinery that determines whether people keep their coverage.
- Reproductive and gender-affirming care: $40 million for reproductive health services and $26 million to maintain access to gender-affirming care.
- Public health infrastructure: $113.3 million to keep the state's disease surveillance and public health IT systems running, and $30 million over five years for Sickle Cell Centers of Excellence.
- The Medi-Cal mobile crisis benefit survives through July 2027 with $42.2 million, though long-term funding for it and the 988 crisis line remains unsettled.
The Legislature also killed two proposed cuts outright: rate caps on PACE, the all-inclusive care program for the elderly, and the elimination of Medi-Cal's acupuncture benefit.
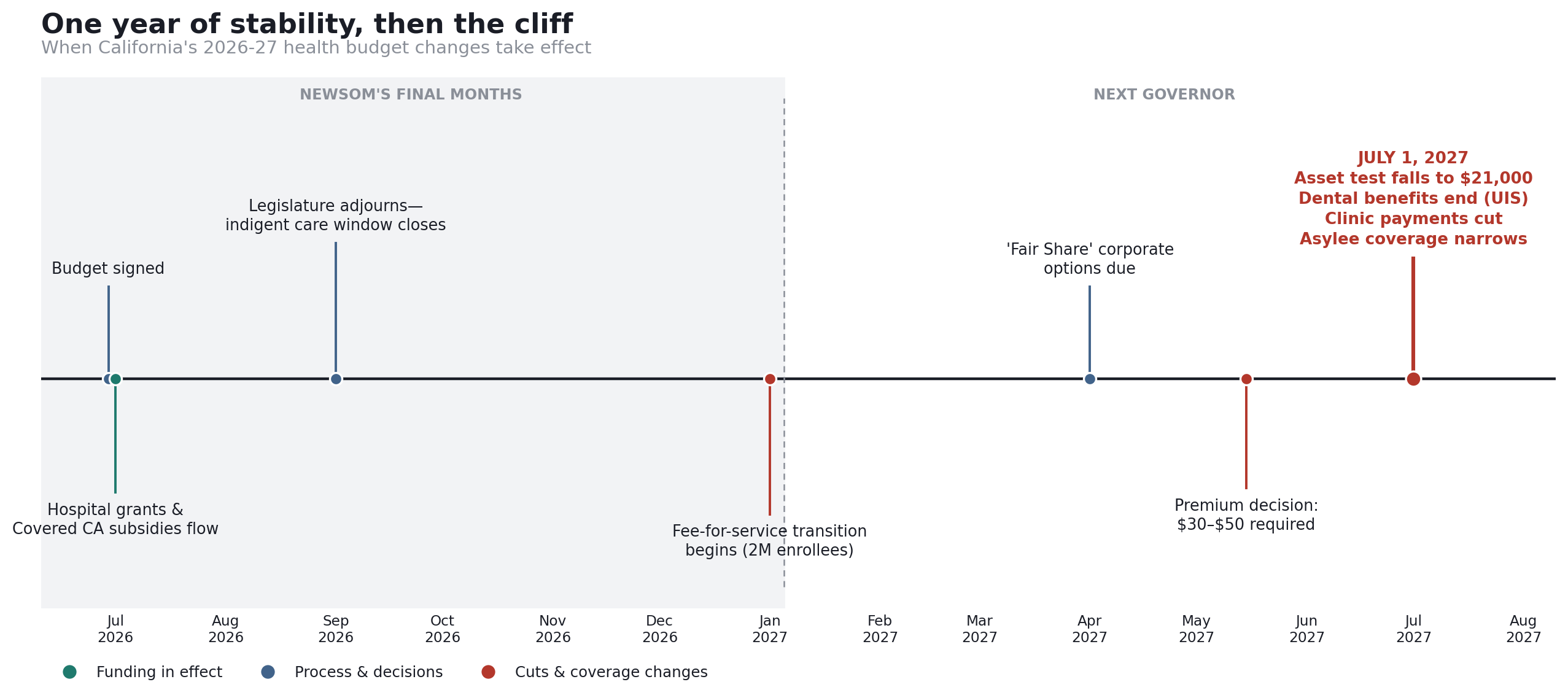
January 2027: 2 million Medi-Cal enrollees move to fee-for-service
The budget's biggest structural change starts before the cuts do. By January, the state begins moving roughly 2 million Medi-Cal enrollees—most of them undocumented immigrants with "unsatisfactory immigration status" (UIS) under federal rules—out of managed care plans and into fee-for-service Medi-Cal.
The administration insisted on the transition to comply with federal directives and preserve federal funding; it saves an estimated $470 million next year. But fee-for-service coverage is thinner in practice. Enrollees lose managed care benefits such as case management, housing assistance, and medically tailored meals, and they'll need to find providers who accept fee-for-service payment. The budget includes $39 million for care coordinators and community-based navigators to help people make the switch.
"While we are relieved this agreement spares immigrant communities from losing access to doctors, dentists and trusted community providers this year, our work is far from over," said Kiran Savage-Sangwan, executive director of the California Pan-Ethnic Health Network.
May 2027: The $30-$50 Medi-Cal premium decision
Newsom's May proposal would have locked in an increase in monthly Medi-Cal premiums for undocumented adult enrollees from $30 to $50. The Legislature refused—sort of.
The final deal keeps premiums at $30 through June 2027, but requires the next governor to set and announce a premium between $30 and $50 in the May 2027 budget revision. The official summaries describe this as preventing an automatic increase. In practice, the increase was converted into a mandatory decision and handed to Newsom's successor, with $50—the number Newsom wanted—written in as the ceiling.
July 1, 2027: Four Medi-Cal cuts land at once
One year from now, the delays run out. Four major changes land on the same day.
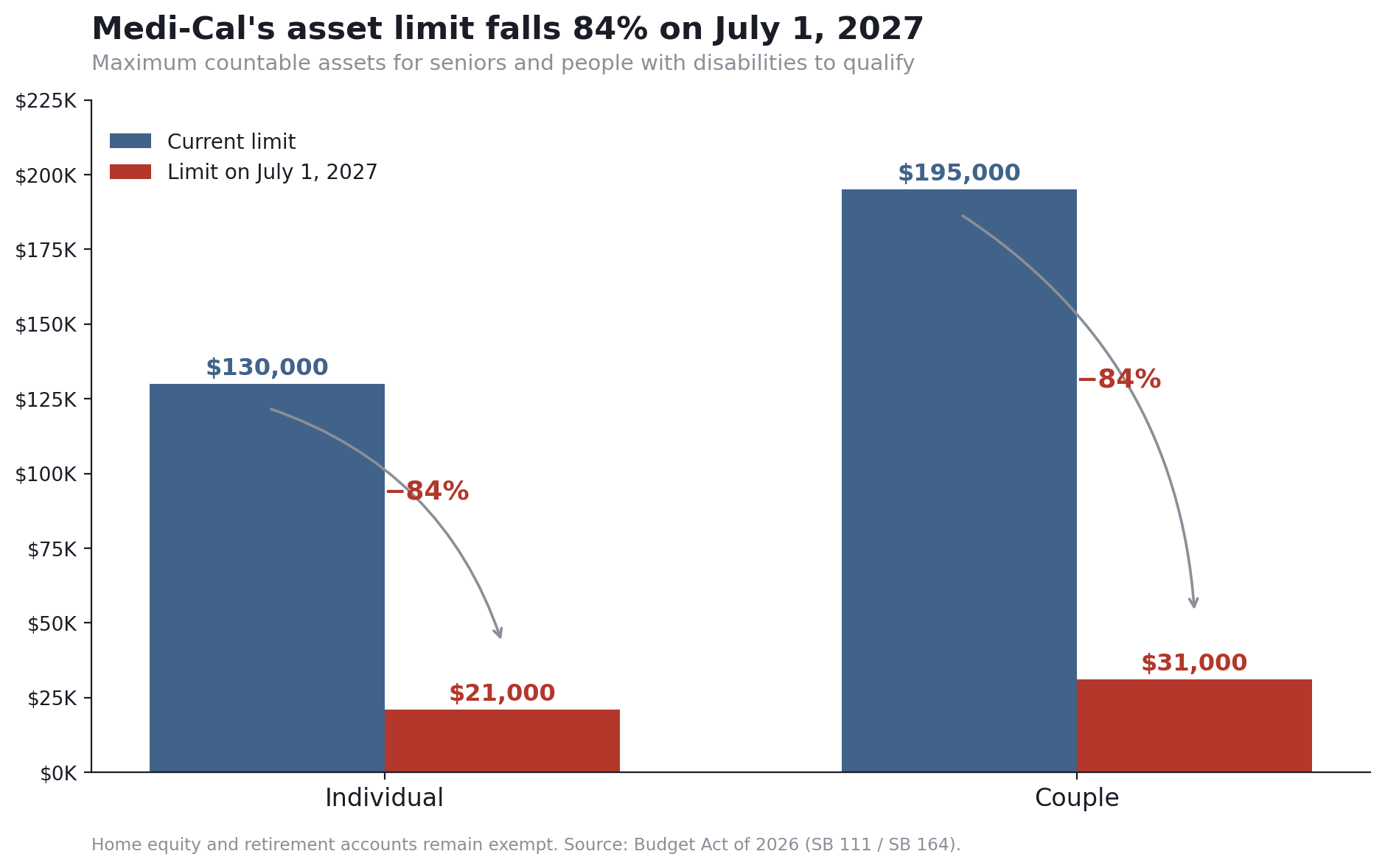
The asset test drops to $21,000
Today, seniors and people with disabilities can qualify for Medi-Cal with up to $130,000 in assets ($195,000 for couples), a ceiling set after the state effectively eliminated the test in 2024. On July 1, 2027, the limit falls to $21,000 for individuals and $31,000 for couples—an 84% reduction.
The official framing celebrates what didn't happen: the Governor's original proposal would have restored the pre-pandemic $2,000 limit immediately. And lawmakers say they'll revisit the number next year. But as enacted, a retiree with $25,000 in savings—roughly one modest emergency fund—loses Medi-Cal eligibility in a year. Home equity and retirement accounts remain exempt; savings, second vehicles, and most other assets count.
Dental benefits end for undocumented adults
Adult dental benefits for enrollees regardless of immigration status—and the Proposition 56 supplemental payments that make dental patients financially viable for dentists to see—were scheduled to end July 1, 2026. The budget buys them one more year. Both expire July 1, 2027 absent new action.
Clinic payments drop
Planned reductions to community clinic and health center reimbursements are also pushed from 2026 to July 1, 2027—at a cost of $1 billion to keep clinics whole for the intervening year. That figure is a measure of what's coming: when the delay lapses, clinics absorb a cut of that scale into their operating reality.
Coverage narrows for asylees and trafficking survivors
Roughly 150,000 immigrants with legal humanitarian status—asylees, refugees, survivors of trafficking and domestic violence—keep full-scope Medi-Cal through 2026-27 (the delay costs $303.2 million). In July 2027, their coverage narrows to emergency and pregnancy care only, unless a future budget intervenes. Legislative leaders say they'll "keep fighting" to reverse this in 2027 "as budget conditions allow."
Left out: The $125 million county indigent care gap
The Legislature wanted $125 million to help counties build an indigent-care backstop—a safety net for people who lose Medi-Cal entirely as H.R. 1's eligibility rules bite. The final budget includes nothing for it.
County associations warn that without an alternative before the Legislature adjourns in September, "counties will be forced to cut core services—threatening public safety, slashing behavioral health and public health services, and driving up homelessness." Counties are the health care provider of last resort under California law; the people falling off Medi-Cal don't stop needing care, they just show up somewhere else on the county ledger.
Who pays: The MCO tax and the corporations clause
Two revenue mechanisms hold the health budget together.
The renewed managed care organization (MCO) tax—a levy on health plans structured to draw federal matching funds—delivers $575 million in General Fund relief in 2026-27 and roughly $2.3 billion annually in the two years after. Voters constitutionally earmarked MCO tax proceeds for Medi-Cal in 2024; this budget's version is rebuilt to comply with new federal requirements.
The more novel provision is the Fair Share from Big Corporations Act. By April 1, 2027, the administration must present the Legislature with "fully viable options" for making large employers pay when their workers rely on Medi-Cal instead of employer coverage—using state wage and enrollment data to identify which corporations those are. If Congress repeals H.R. 1's Medicaid cuts, the requirement pauses. It's a study clause today; it's designed to become next year's tax fight.
What to watch: Key dates through July 2027
Final word: A one-year lease on the status quo
Measured against January's proposals, this budget is a rescue: no immediate asset test collapse, no dental cliff this year, hospitals get real money, and the safety net's administrative spine gets funded. Measured against what the law now schedules for July 1, 2027, it's a countdown. The same budget that spares Medi-Cal this year formally enacts most of the cuts it celebrates avoiding—it just moves the effective dates past the next election.
California's health care system has one year of purchased stability. What happens after depends on three things this budget deliberately left open: the revenue forecast, the next governor, and Congress.
Frequently asked questions
Is Medi-Cal being cut in California?
Mostly not yet—but most cuts are scheduled. The 2026-27 budget delays the largest Medi-Cal reductions (dental benefits, clinic payments, the asset test, and immigrant coverage changes) until July 1, 2027, and rejects a few outright, including PACE rate caps and the elimination of acupuncture coverage.
When does the Medi-Cal asset test change?
July 1, 2027. The current limits—$130,000 in assets for an individual and $195,000 for a couple—drop to $21,000 and $31,000. Home equity and retirement accounts remain exempt. Lawmakers have said they will revisit the level in next year's budget.
Will Medi-Cal premiums go up for undocumented enrollees?
The $30 monthly premium holds through June 2027. The next governor is required to set a premium between $30 and $50 in the May 2027 budget revision, taking effect July 1, 2027.
What is the Medi-Cal fee-for-service transition?
By January 1, 2027, roughly 2 million enrollees with "unsatisfactory immigration status" move from managed care plans to fee-for-service Medi-Cal, preserving federal funding but ending benefits like case management, housing assistance, and medically tailored meals. The state funded $39 million in navigators to help enrollees through the switch.
What do hospitals get in the 2026-27 California budget?
$250 million in grants for designated public hospitals and $90 million for hospitals in significant financial distress (augmentable by up to $50 million), plus $10 million for a new state unit that helps struggling hospitals maintain services. Hospital groups had requested $500 million.
Budget Act of 2026—Official Senate Summary
The Senate Budget and Fiscal Review Committee's official summary of the 2026-27 agreement (June 26, 2026). PDF.



